Meniscus Tears and Knee Arthroscopy
Overview

General Information
- Meniscus Tears don’t always hurt
- Anatomy
- Types of Meniscus Tears
- Cause of Meniscus Tears
- Diagnosis of Meniscus Tears
- Meniscus Tears and Arthritis
- Treatment for Meniscus Tears
- What is Knee Arthroscopy?
- Recovery after Surgery
Many patients have meniscus tears that are not, in fact, causing their knee pain. There are many other causes of knee pain other than a meniscus tear. Many orthopaedic surgeons and sports doctors see patients with MRI findings of a meniscus tear and knee pain but, after a careful physical examination it is found that the meniscus tear is unlikely leading to the patient’s pain. In fact, many meniscus tears do not cause any pain at all.
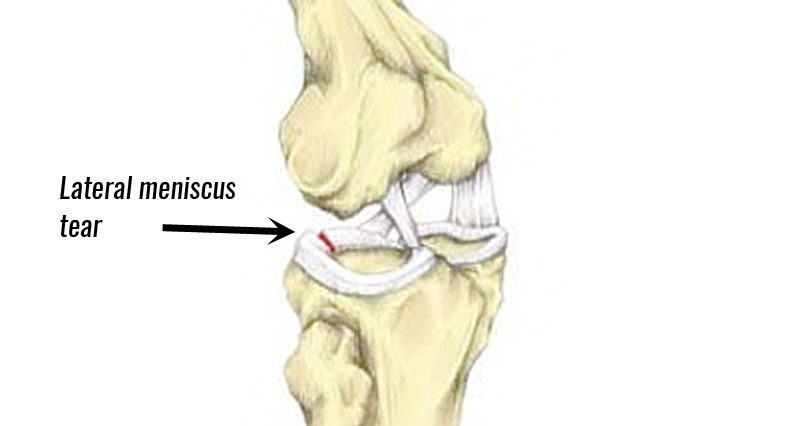
The meniscus is horseshoe-shaped piece of cartilage that sits in between the tibia and femur in the knee. It acts like a “cushion” to dissipate contact forces between the two bones. Each knee has two menisci. There is a meniscus on the inner part of the knee “medial meniscus” and a meniscus on the outer part of the knee “lateral meniscus”.
{kind=link}
The blood supply of the meniscus is better in the peripheral part (red zone) and poor in the central part (white zone). Because of this, the meniscus does not heals better in the peripheral part compared to the central part. Attempting to repair meniscus tears in the central portion usually results in failure of the repair. That is why meniscus tears central part are usually trimmed. Meniscus tears in the peripheral part of the meniscus are sometimes repairable.
- Degenerative/horizontal/complex tears – This is the most common type of tear, caused by age or arthritis. These types of tears are successfully treated with physiotherapy most of the time.
- Flap or Parrot Beak tear – Can cause intermittent feeling of locking or pain. In between episodes, can be painless. If physiotherapy does not resolve symptoms, see an orthopaedic surgeon
- Vertical/Longitudinal – Often associated with ACL tears. This kind of tear may heal on its own or may be amenable to surgical repair or removal of the torn portion.
- Bucket Handle tear – A special kind of longitudinal tear where the torn piece has moved into a spot that blocks full straightening of the knee. If you are young and have just sustained this kind of injury, seek a referral to an orthopaedic surgeon as soon as possible.
Intrasubstance / Non Surfacing Tears – This is not a true tear, but a precursor to a tear. It is a change in the consistency of the meniscus within the substance of the meniscus itself, as noted on an MRI report. It is not usually the cause of the patient’s knee pain. It can not be visualized during surgery, so treatment for this issue is only non-surgical (physiotherapy).
- Injury (often twisting of the knee)
- Degenerative changes (wear and tear) due to
- Age
- Arthritis (one of the most common causes) (see below)
- Obesity
- Chronic ACL tear
Often a specific injury can make a previously painless degenerative meniscus tear painful.
If your doctor suspects a meniscus tear, you need to have standing x-rays of your knee first to look for arthritis. If your knee x-ray is normal and your doctor suspects a meniscus tear as the cause of your pain, then an MRI is required to make the definitive diagnosis. A knee ultrasound does not do a good job in identifying clinically significant meniscus tears.
If you have knee pain and obvious arthritis on x-ray, you do not need an MRI to look for a meniscus tear. You need to be treated for your knee arthritis.
Most patients with knee arthritis have meniscus tears. There is good evidence to suggest that performing knee arthroscopy on meniscus tears in patients with knee arthritis does not help. In fact, knee arthroscopy for “a cleaning” in patients with known knee arthritis, is no longer funded by the Ontario Ministry of Health.
Physiotherapy
The initial treatment for most meniscus tears is physiotherapy. This would entail an active-based strengthening program, taught to you by a physiotherapist. The program should concentrate on decreasing your swelling, increasing your range of motion and strengthening your quadriceps and hamstrings.
Physiotherapy can lower or eliminate the pain from meniscus tears, but can not directly heal the meniscus tear itself. Many patients can become pain-free after doing physiotherapy for meniscus tears. If you do not have pain from your meniscus tear, then no further treatment for those tears is typically necessary.
Injections
For degenerative tears associated with arthritis, various types of injections can be considered to help with the pain. Note that injections typically act by lowering inflammation. Injections are not known to “heal” a torn meniscus.
See Section on Injections.
Knee Arthroscopy
Candidates for Surgery
Surgery for meniscus tears is considered for patients who
- Do not have significant arthritis on standing xrays of their knee
- Have tried 6 months of physiotherapy
- Have a meniscus tear that can be either trimmed or repaired
Surgery is also considered expeditiously in the special case of a young patient with a displaced, bucket-handle meniscus tear causing a “locked knee”.
Meniscus surgery is done entirely or is assisted arthroscopically. An “arthroscope” is a camera on a long, skinny lens, designed to go inside a joint. The surgery is typically done under a general anesthetic. During surgery, your orthopaedic surgeon will make 2 or 3 small incisions in the knee to allow for the passage of 1) the scope, 2) specially designed instruments and 3) water management. (During knee arthroscopy, orthopaedic surgeons inflate the knee a little with water to allow for easier passage of the camera and instruments.) Each incision is about 5mm in size (a fifth of an inch).
Meniscal trimming
Most tears in the central 2/3 of the meniscus need to be trimmed by special instruments so that the torn part does not continue to move around within your knee. It is hypothesized that this loose part of the torn meniscus is what’s contributing to the pain. Since meniscus is part of the cushioning of the knee, only the torn portion of the meniscus is removed (“partial meniscectomy”). In theory, this torn portion is no longer doing its job cushioning the knee and could be causing pain.
Meniscal Repair
Occasionally, in young patients, unstable longitudinal and bucket handle tears in the peripheral portion of the meniscus can sometimes be repaired. Sutures are placed to stabilize the meniscus, in hopes that the body then heals the meniscus. If the meniscus does not heal, and the meniscus tear becomes unstable again, it can cause a feeling of locking and a second surgery to remove the torn part of the meniscus is required.
If a bucket handle meniscus tear is old, the piece that is displaced can shrink or get shredded lowering the possibility of performing a successful meniscal repair. It is for this reason that young people with a displaced bucket handle meniscus tear see an orthopaedic surgeon as soon as possible.
Patients who undergo partial meniscectomy or meniscal repair are discharged from hospital the same day of surgery.
Patients who have had a partial meniscectomy are allowed to put full weight on their leg immediately after surgery and are usually able to walk without crutches immediately after surgery. Patients who have had meniscal repair are instructed to partially weight-bear on the operated leg for six weeks after surgery, so will need crutches during that time.
Physiotherapy after Meniscectomy or Meniscal Repair
It is important that you see your physiotherapist within a few days after your surgery in order to decrease your swelling and improve your range of motion and quadriceps strengthening. During your sessions, your therapists should be teaching you exercises that you can do on your own. Your therapist should observe you doing the exercises you have already been taught, correct any issues, and teach you new exercises. You are expected to do those exercises as instructed by your therapist most days of the week on your own. The further along in your recovery, the less often you need to see your physiotherapist.
- Partial meniscectomy (meniscal trimming) – approximately 6 weeks of physiotherapy recommended
- Meniscal repair (without ACL reconstruction) – approximately 12 weeks of physical therapy is recommended. This is because patients are limited to partially weight-bearing during the first six weeks after meniscal repair.
Navigating the System
How to get an appointment with Dr. Cayen
- See your Family Doctor
The first step in the Canadian Health Care System is to see your family doctor. Your family doctor will ask you questions and do a physical exam.
- Get Some Imaging of your Knee
If necessary, your family doctor will order x-rays (if they have not already been done) to look for arthritis. If you have obvious arthritis on x-ray, then an MRI is not necessary. You need treatment for your knee arthritis. If there is no arthritis on xray and your family doctor suspects a meniscus tear, then an MRI will be ordered.
- Start Physiotherapy
While you are waiting for your MRI, you should start some physiotherapy for a presumed meniscus tear. Your family doctor can give you a prescription for that.
- Obtain a Referral from your Family Doctors
If physiotherapy does not help your symptoms and you are interested in having a knee scope for your meniscus tear, your family doctor can refer you to an orthopaedic surgeon, like Dr. Cayen, who performs this procedure. You can request that your family doctor refer you to an orthopaedic surgeon of your choice.
If you have been referred by one of Humber River Hospital Emergency Department physicians, an extra visit to your family doctor for a referral is not necessary.
- Your Appointment with Dr. Cayen
What do I bring to my appointment?
- X-ray and MRI Disks : If you did not have an x-ray or MRI performed at Humber River Hospital, you must bring the disks of your x-ray and MRI with you to the appointment. Although Dr. Cayen may have received the reports from your referring physician, he needs to see the actual images found on the disks.
- Why do I need both an x-ray and MRI? Isn’t that redundant?
- A standing xray of your knee clearly shows how much arthritis there is in the knee. An MRI does not do a great job of showing “joint space narrowing” that exists with arthritis. If you have significant arthritis, then a knee scope for a meniscus tear is not appropriate.
- The MRI shows the configuration of the meniscus tear if surgery for your type of meniscus tear is appropriate.
- So both the x-ray and MRI help Dr. Cayen figure out what treatment is best for you.
- Why do I need both an x-ray and MRI? Isn’t that redundant?
- A pair of shorts: Dr. Cayen will need to examine your knee. He can’t do that through pants.
- Intake Form: Print and fill out this intake form. Give it to Dr. Cayen when you meet him.
Preparing for Surgery
- General Health
Smoking
Stop smoking at least 6 weeks prior to your surgery. Smoking inhibits bone and soft tissue healing. Smoking can increase the risk of poor wound healing and increases the risks of infection after surgery. Smoking can increase the risk of lung complications after a general anesthetic. Resources for smoking cessation can be found here.
Diabetes
If you have diabetes, getting your blood sugars under control prior to your surgery is important. Before your surgery, speak to your family doctor or endocrinologist about your “Hemoglobin A1c”. If it is high, it might mean that your blood sugars are not under control. Poorly controlled diabetes increases the risk of infection after knee surgery.
Strengthening Exercises
Seeing a physiotherapist once or twice immediately after your injury can help
- Lower your swelling
- Improve your range of motion and
- Re-activate your quadriceps to get you back walking normally.
- Discharge Planning
After knee arthroscopy, you will be discharged home the same day of surgery.
You will need
- A ride home from the hospital, pre-arranged by you.
- Assistive Devices
If you have a partial meniscectomy (meniscal trimming), you will not need crutches. You will be allowed to put full weight on your operated leg immediately after surgery
- If you have a meniscal “repair”, you will need crutches for 6 weeks after your surgery as you will be restricted from putting full weight on the operated leg for that amount of time. Bring your crutches to the hospital on the day of your surgery, so that our physiotherapists can adjust them for you and teach you how to use them.
- Dr. Cayen recommends the use of a cold-compression device (cryotherapy) for pain control after your surgery. This may be covered by many extended-health insurance policies. Dr. Cayen’s administrative assistant will speak to you about cryotherapy prior to your surgery.
- Day of Surgery
Do not eat or drink anything after midnight the night before surgery. You should take the medications you have been instructed to take the morning of surgery with sips of water. Do not take the medications you have been told to stop taking.
Arrive at Humber River Hospital 2 hours before your scheduled surgery. Take the Central Elevators to the 2nd floor. Go to the Surgery Registration desk on the 2nd floor. You will be registered, then get changed into a gown. (Wear briefs, not boxers. Underwear that covers the thigh will need to be removed). You will have an intravenous line started and may be given some medications for pain and nausea. You will then see our anesthesiologist who will discuss the anesthetic. Typically, knee arthroscopy is done with a general anesthetic and local anesthetic during the procedure.
Recovery
- Initial Recovery
Same-day discharge from hospital
You will recover initially in the post and aesthetic care unit (PACU). You will then complete your recovery in the Surgical Day Care (SDC) unit. You will be discharged home on the same day of your surgery. You will need a ride home after your surgery.
- Prescriptions
You will be discharged home with a prescription for painkillers and a stool softener (if needed). You will also be given a prescription for post-operative physical therapy. Prior to your surgery, arrange to start your physiotherapy 3-5 days after your procedure.
- Follow Up Appointments
You will see Dr. Cayen 1-2 weeks after your surgery. He will check your wound and make sure you are doing your home exercises. Dr. Cayen will check your knee range of motion. Your sutures will be removed, if you have them. Your subsequent follow-up with Dr. Cayen will be at approximately the 6-week mark. If you have a meniscal repair, a 3-month visit is arranged.
All follow-up appointments occur in the Fracture Clinic at Humber River Hospital.
If concerns regarding your knee arise between your scheduled visits, please give Dr. Cayen’s Administrative Assistant a call.
- Wound Care
Our nurses will give you instructions on wound care. Keep the wound dry until the wound heals completely. Do not submerge the wound under water (eg in a tub or swimming pool) until the wound is completely closed (usually around 3 weeks after surgery).
- Driving
For right-leg surgery, you can drive once you are not using crutches and are not using narcotics for pain control.
For left-leg surgery, if you are driving an automatic transmission vehicle, you can drive once you are no longer taking narcotics for pain control. If you drive a standard transmission vehicle, the restrictions are similar to right-leg surgery.
You need to feel confident that you can hit the break with good force and reaction time before you return to driving.
- Work and Activities
Return to work depends on the kind of job you have. Dr. Cayen suggests working not more than 2-3 hours per day during the first few weeks after surgery and to take frequent breaks. Sitting for long periods of time after knee surgery can theoretically increase the risk of blood clots. Spend your first few weeks after surgery doing your physiotherapy and resting.
School: It is reasonable to take about a week off school after knee arthroscopy. After that time, you will be able to attend most of your classes unless they involve prolonged standing/walking or physical activity.
Sedentary/Desk job: It is reasonable to take 1-2 weeks off of a sedentary job after knee arthroscopy. Many patients start working from home after a few days (as long as they are not taking narcotics for pain).
Jobs involving walking or lifting: Typically patients can get back to an active job approximately 4-6 after a partial meniscectomy. This changes to about 3 months after meniscal repair. When you do return to work, Dr. Cayen suggests return to work gradually, with graduated hours and graduated duties over a number of weeks.
Return to Sport
If you dutifully perform your physiotherapy after your knee arthroscopy (including a home- or gym-based strengthening program), you may be able to return to sport approximately 6 weeks after partial meniscectomy and about 3 months after meniscal repair surgery.
Your physiotherapist will test out your leg strength before allowing you to return to sport. These tests include one-legged quadriceps and hamstring strength (3 rep max) and hop tests. Your operated leg needs to be 90% as strong as your non-operated leg before returning to sport.
Importantly, your physiotherapist or athletic therapist needs to train you on agility and sport-specific drills before you return to sport safely.
DISCLAIMER: The information on this website is intended to help current and prospective patients of Dr. Cayen understand joint disease as well as treatment options available. It is also meant to provide background information to prospective patients such that their visit with their doctor is most helpful. This website is not meant to provide specific medical advice, treat or diagnose any medical condition. It is not meant to take the place of a visit with your doctor or Dr. Cayen.
About Dr. Cayen
Dr. Barry Cayen is an orthopedic surgeon at Humber River Hospital, specializing in adult hip and knee replacements, sports surgery of the knee, and trauma. He performs Total Hip Replacement Surgery using the Direct Anterior approach with a Hana table.