Direct Anterior Hip Replacement
Overview

Frequently Asked Questions
- What is Hip Arthritis?
- What Non-Surgical treatment exists for Hip Arthritis?
- When is Hip Replacement Suggested?
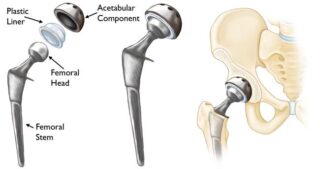
- What gets “Replaced” during a Hip Replacement?
- What is the Anterior Approach?
- What are the risks of hip replacement surgery
The hip is a ball and socket type joint. With arthritis, the smooth cartilage coating on the femoral head (ball) and acetabular (socket) surfaces is worn away and underlying bones rub together.
Patients with hip arthritis often feel:
- Groin or buttock pain with walking
- Groin or buttock pain while getting up from a seated position. Many patients feel that their hip needs to “loosen up” before they can start walking (“start-up pain”).
- Hip stiffness, making sitting or putting on socks or shoes difficult
Hip Arthritis can be caused by:
- Osteoarthritis (wear and tear with age or obesity)
- Rheumatoid arthritis or other inflammatory arthritis
- Hip dysplasia (shallow hip socket from birth)
- Avascular necrosis (eg from chemotherapy, previous prednisone use, sickle cell disease and other causes
- Previous hip fracture
- Previous hip infection.
The initial treatment for hip arthritis can include:
- Pain medication – unless you have liver problems, acetaminophen (Tylenol) is typically recommended, to start. Many medical associations have recommended AGAINST using narcotics for arthritis pain, as this can risk addiction, without an improvement in pain.
- Anti-inflammatory medication – ask your family doctor if you may safely take anti-inflammatory medication. Patient with a history of stomach ulcers, high blood pressure, or kidney disease should usually avoid these types of medication.
- Physiotherapy – visit a physiotherapist so that they can teach you a program focused on quadriceps, hamstrings and abductor strengthening that you can do at home, on your own. See your physiotherapist occasionally so that they can monitor your progress, correct your form, and add exercises to your program. If you are being funded by extended health benefits and you are on a waitlist for surgery, be sure to save most of your benefits for after surgery.
- Walking aids – a cane or walker may help walking be more comfortable
- Hip injections – a good non-operative option. See section on injections
- Weight-loss, if necessary. If you are overweight, losing as little as 20 pounds can improve your hip pain. Although exercise is important for strong muscles and heart health, diet is, by far more important for weight loss. Speak to your family doctor about diet resources. You can get started with information regarding healthy eating at the Heart and Stroke Foundation of Canada.
If non-surgical treatment does not adequately manage hip arthritis pain, then total hip replacement can be considered.
No amount of online information can replace a visit with an orthopaedic surgeon to determine if you would benefit from a hip replacement. This serves as a guide only. Hip replacement is an option in patients who have evidence of hip arthritis and
- hip pain due to the arthritis that significantly limits walking or other everyday activities. Hip arthritis is only one of the many causes of pain around the hip. (Other causes of hip pain include back issues, tendon, muscle, or other soft tissue problems.)
- tried non-surgical options that have not adequately helped with their pain/function
- good underlying health. Patients who have had recent cardiac events, heavy smokers, poorly controlled diabetes, morbid obesity or dementia, are at high risk for complications after hip replacement surgery.
Hip replacement surgery replaces the femoral head with an artificial ball. The ball is “potted” into the thigh bone with a metal stem. A metal shell and plastic liner is inserted into the acetabulum (socket). This acts to replace both the ball and socket of the hip and helps alleviate the pain from hip arthritis.
The anterior approach to hip replacement is gaining popularity because the recovery for patients is faster during the first 12 weeks after surgery, compared to other approaches. The “approach” means the direction a surgeon can take to get to the area of interest. Hip replacement can be “approached” from the back (posterior), side (lateral) or front (anterior). The anterior approach is a muscle-sparing approach that goes between muscle groups, rather than through them or having to detach major tendons.
It is important to note that there is no difference between the approaches in terms of the implants used or the long-term outcome of hip replacement. No approach is pain-free, so patients do need to expect surgical discomfort after any hip replacement. This discomfort dissipates significantly over the first 2 weeks post operatively.
Most of our patients after Anterior Hip Replacement are able to walk with a walker and do stairs within a few hours of surgery. Because the immediate surgical pain after the Anterior Approach is so much less compared to other approaches, most of our patients after Anterior Hip Replacement are able go home the same day of surgery.
We use a special operating table called the “Hana Table” for Anterior Hip Replacements. It allows us move your leg easily and to check our work using low-dose x-ray during the procedure, if necessary.

Rarely, patients are not candidates for the anterior approach (patients with ankylosing spondylitis, skin infection near the incision site and some revision surgery).
Skin Numbness
Most patients experience a patch of skin numbness, about the size of their hand just beyond the incision site of an anterior hip replacement. This patch of skin numbness will not affect your function.
Leg Length differences
Often after hip replacement, the operated leg is slightly longer than before surgery. This is often favourable because arthritic hips are often shorter than non-arthritic hips. Dr. Cayen will use either x-ray or computer navigation technology during your hip replacement surgery in an attempt to make leg lengths as even as possible during surgery. A leg length difference of more than 2cm after surgery is very rare, unless there was a significant leg length difference before surgery. Many leg length differences immediately after surgery “even out” with time as the pelvis adjusts.
Blood Loss
Some blood loss during hip replacement is normal. Blood loss requiring a blood transfusion after surgery is rare unless you are anemic (low hemoglobin levels) before surgery or you are having both your hips replaced at once. You will be sent for blood work when you book your surgery to make sure that you are not anemic. If you are anemic before surgery, we will refer you to our Patient Blood Management Coordinator who may suggest ways to build up your hemoglobin levels prior to your surgery.
Infection
The lifetime risk of a serious infection after a hip replacement is approximately 1%. Some of these infections occur soon after surgery, but most occur months or years afterwards. The treatment for serious (deep) infections includes revision surgery and IV antibiotics.
More commonly, patients can get less serious skin infections “cellulitis”, which can often be treated with antibiotics that can be taken by mouth. Sometimes surgeons will opt to “wash out” a skin infection in the operating room if the cellulitis gets serious.
People at higher risk for infection include patients with poorly controlled diabetes, patients with morbid obesity (BMI more than 40), patients who are immunocompromised, or are taking immunosuppressant drugs, patients with peripheral vascular disease and smokers. An ongoing infection at the time of surgery from another source (eg active urinary tract infection, tooth abscess, diabetic foot infection) can increase your risk of infection after surgery.
In order to prevent infection, your surgeon will give you one dose of antibiotics through your IV in the operating room before your surgery. You will get another dose after your surgery. Growing evidence suggests that prolonged administration of antibiotics after your surgery does not prevent infection.
The symptoms of infection include fevers, redness around the wound, persistent leaking from the wound and increasing pain in a previously well-functioning joint replacement. If you think you are developing an infection around your hip replacement, call your orthopaedic surgeon’s office as soon as possible or go to your nearest emergency department.
Blood Clot
Blood clots in leg veins can occur after hip surgery. Your surgeon will prescribe a medication for you to take after your surgery in order to prevent blood clots. If a clot develops in a deep leg vein (deep vein thrombosis – DVT) above the knee, it will need to be treated with stronger blood thinners. Above knee DVTs need to be taken seriously because they can cause clots that go to the lungs (pulmonary embolus), which is a serious condition. If you have previously had a DVT, please let your surgeon know prior to your surgery.
Pain after Hip Replacement
It is normal to have some soreness in the hip after anterior hip replacement. This soreness typically improves significantly over the first 6 weeks after surgery. Many people still experience soreness up to 3-6 months after surgery. Barring complications, hip replacement surgery can help with 85-90% of hip pain at the 3-month mark. It is important to know that although most patients enjoy improved function, improved mobility and significant pain relief after recovery, a hip replacement does not typically feel like a “normal” hip.
Dislocation
Although unusual, hip dislocation is when the ball of the hip replacement comes out of the socket. If this happens, you will know that something is wrong and will need to go to your nearest emergency department to have the hip put back into place. The most common reason this happens is bending forward or twisting awkwardly. Other reasons for hip dislocation include infection, component malposition and shortening of the leg after surgery. The risk of dislocation is highest in the first 3 months after surgery. Recurrent hip dislocations sometimes require revision surgery. The risk of hip dislocation after the anterior approach is theoretically lower than the risk of dislocation after the posterior approach.
Component loosening
The metal components of the hip replacement are meant to bind with your bone in the first 3-6 months after surgery. Over the years however, this bond can loosen, requiring a revision of the components. Less common causes of early loosening include infection or failure of the components to bond to bone after implantation.
Damage to Blood Vessels or Nerves
Damage to major blood vessels or nerves causing permanent muscle weakness is exceptionally rare, especially from the anterior approach.
Navigating the System
Appointments Before Hip Replacement
- Family Doctor
If you are wondering if you need a hip replacement, the first step in the Canadian Health Care System is to see your family doctor. Your family doctor will ask you questions, do a physical exam and order x-rays, if they think it’s necessary. If your x-rays show arthritis, and you are interested in a hip replacement, then your family doctor can refer you to an orthopaedic surgeon, like Dr. Barry Cayen, who performs hip replacements. You can request that your family doctor refer you to an orthopaedic surgeon of your choice.
- Central Intake Clinic
For patients living in Ontario, Dr. Cayen’s hip and knee arthritis referrals are fast-tracked to a Central Intake Clinic, where patients are initially seen by an Advanced Practice Physiotherapist (APP). The APP will perform a physical exam, review x-rays with you and educate you about hip replacements, if you’re a candidate. If you are interested in surgery and are a candidate, you will then have an appointment made with Dr. Cayen, usually on a different day. Although seeing the APP might seem like an extra step, the feedback we get from patients is that they learn a lot about the procedure during that visit and find it helpful. Dr. Cayen reserves slots for patients who have been seen by the APP, so the wait to see him from the time of the initial referral from the family doctor (Wait 1) is not lengthened in the process.
- Dr. Cayen
When you see Dr. Cayen, he will ask you some questions about yourself, perform a physical exam on your hip and review your x-rays. If you, together with Dr. Cayen decide to proceed with hip replacement, you will sign consent for surgery, attesting that you understand the risks and benefits of surgery. You will then complete some blood work, if it has not already been done recently (CBC, electrolytes, Creatinine, Vitamin B12, Iron panel). Dr. Cayen’s Administrative assistant will call you over the subsequent months to discuss your surgical date. At that time, you may ask Dr. Cayen’s Administrative Assistant to be placed on a “cancellation list” if you are able to go ahead with your surgery on short notice.
- Surgical Pre-Screening
You will have a Surgical Pre-Screening Appointment at the Hospital up to 1 month prior to your surgery. There, you will see a nurse who will review your medications (please bring them with you). You will also see an anesthesiologist. You may also see a physiotherapist. You should have a discharge plan in place prior to your surgical pre-screening appointment. You will receive a text, email or telephone notification with the date and time of your appointment. Please refer to your surgical package for other important information.
- Internal Medicine
A separate Internal Medicine appointment may be necessary. We will let you know if that is the case.
- Your other Treating Physicians
You may need to follow up with your family doctor or your other treating physicians (endocrinologist, cardiologist, rheumatologist, if you have one) prior to your surgery to discuss your suitability for an elective hip replacement or to discuss changing or temporarily stopping some of your medications prior to surgery.
Preparing for Surgery
- Discharge Planning
Most of our patients at Humber River Hospital who undergo Anterior Hip Replacement are discharged home the same day of surgery. Patients are encouraged to start discharge planning as early as possible in the process (even before they meet Dr. Cayen). All patients undergoing anterior hip replacement should plan to be discharged from hospital the same day. The remainder of patients go home the next day, depending on underlying medical conditions or post-operative issues may that arise.
You must plan to be discharged from hospital to a place where someone can help you the evening of surgery, and for the subsequent 2 to 3 days. You may be discharged back to your own home or to a family member or friend’s place after surgery, as you have arranged. You should let Dr. Cayen know your discharge plan during your visit with him.
If you do not have a place where you can be monitored after your surgery, you may choose to consider respite care at a short-stay retirement home. Respite care must be arranged by you well in advance of the surgery date. Respite care is an out of pocket expense. A sample list of respite care locations can be found here.
For final questions regarding your discharge planning, you may ask to speak with a Social Worker or our Orthopaedic Care Navigator.
- Do I continue taking my regular medication?
Do not stop or change any medications before speaking with your doctor. The information below is meant only to give you an idea of what to expect before your surgery.
– Inflammatory Arthritis Medications
If you are taking medications for inflammatory arthritis (such as Rheumatoid Arthritis), you may need to stop some of those medications for a few weeks before and after your surgery. Many Disease Modifying Antirheumatic Drugs can increase the risk of infection around the time of surgery and can seriously affect wound healing. Let Dr. Cayen know if you are taking any such medications. You will need to speak with your Rheumatologist before stopping these medications temporarily. A scientific review paper on this topic, accessible by your Rheumatologist can be found here.
– Blood Thinners
If you are taking blood thinners by mouth, you may need to stop taking those for up to a week prior to your surgery. Let Dr. Cayen know if you are taking any such medications. You will need to speak with your Family Doctor before stopping these medications temporarily.
– Diabetic Medications
If you have diabetes, you will be seen by an internal medicine specialist prior to your surgery who will tell you which of your diabetes medications should be changed temporarily prior to your surgery. You may need to speak with your Family Doctor or Endocrinologist before adjusting these medications temporarily.
– Narcotics
If you are taking narcotics for chronic hip pain or other chronic musculoskeletal pain, Dr. Cayen suggests that you work with your prescribing physician to slowly lower or eliminate the use of those medications. Patients who are taking narcotics prior to surgery have a more challenging course with pain control after surgery.
Information for patients on opioid tapering can be found here.
Information for physicians regarding opioid guidelines can be found here.
- Obesity, Smoking, Diabetes control
Weight Control and Diet
- Being overweight can put excessive forces through hip replacements and may lead to early loosening of the implants. Scientific data suggests that if your Body Mass Index (BMI) is more than 40, you are at increased risk of infection after hip replacement. Excessive weight can compromise optimal component position during surgery. Decreasing your weight, if necessary can improve your hip pain prior to surgery and improve the speed of recovery after surgery.
-
- Calculate your BMI here
ft
in
lbs
cm
kgBMI
-
Although exercise is important for weight control, diet is by far more important. Some things you can do to help with your diet include lowering overall portions, eating food high in protein and lower in carbohydrates, not eating after dark, not drinking beverages with calories (such as soft drinks or fruit juices) and creating a food diary. Speak to your family doctor about a weight loss program, if necessary. One resource for weight loss from the Heart and Stroke Foundation can be found here.
Smoking
Stop smoking at least 6 weeks prior to your surgery. In addition to damaging your lungs and heart, smoking slows bone healing which is an important part of having the implants in joint replacement surgery bond to your bone. Smoking will make your recovery from surgery take longer. Smoking also increases the risks of poor wound healing and increases the risks of infection. Resources for smoking cessation can be found here.
Diabetes
If you have diabetes, getting your blood sugars under control prior to your surgery is important. Before your surgery, speak to your family doctor or endocrinologist about your “Hemoglobin A1c”. If it is high, it might mean that your blood sugars are not under control. Poorly controlled diabetes increases the risk of infection after hip replacement surgery.
Strengthening Exercises
Seeing a physiotherapist once or twice before your surgery to teach you hip strengthening exercise may be helpful to quicken your recovery after surgery. The stronger you are before your surgery, the stronger you will be afterwards and the faster your recovery will be.
- Assistive Devices
Prior to your hip replacement surgery you are encourage to gather the following items.
- 2-wheeled walker. – You will need a walker for 1-3 weeks after your surgery.
- Cane. – You will progress to using a cane after the walker. You may need a cane for up to 12 weeks post operatively. Everyone’s progress through their requirement of walking aids is different.
- Raised toilet seat. – Might be more comfortable for you for the first 12 weeks after surgery
- Non-slip bath mat
- Dr. Cayen recommends the use of a cold-compression device (cryotherapy) for pain control after your surgery. This may be covered by many extended-health insurance policies. Dr. Cayen’s administrative assistant will speak to you about cryotherapy prior to your surgery.
- Day of Surgery
Do not eat or drink anything after midnight the night before surgery. You should take the medications you have been instructed to take the morning of surgery with sips of water. Do not take the medications you have been told to stop taking.
Arrive at the Hospital 2 hours before your scheduled surgery. If you are having your surgery at Humber River Hospital, take the main elevators to the second floor. Go to the Surgical Registration desk. You will be registered, then get changed into a gown. You will have an intravenous line started and may be given some medications for pain and nausea. You will then see our anesthesiologist who will discuss local anesthetic, spinal anesthetic or general anesthetic, depending on your needs.
Recovery
- Initial Recovery
You will wake up and recover initially in the Post Anesthetic Care Unit (PACU) where xrays of your new hip will be taken. You will then be moved to our Surgical Day Care (SDC), where you will complete your recovery, receive some medications and be seen by our physical therapists (PTs). Our PTs will get you up walking in the SDC within a few hours of your surgery. You will be allowed to put full weight on your leg after surgery. When our PTs deem you’re safe for discharge home and your pain and nausea are under control, you will be discharged home with family or friends the same day of surgery. You must arrange to get a ride to and from your surgery ahead of time.You will be discharged home with prescriptions for pain killers, a blood thinner and a prescription for post-operative physical therapy.You may need a walker for approximately 2 weeks after your surgery. You may need to use a cane up to the 6-8 week mark after your surgery. Everybody’s recovery pace is different. As long as you are improving week-to-week, you are doing well.
- Pain Control
Our pharmacy will put together a combination of pain medications in a blister-pack for you to help manage your discomfort after surgery. Inside this blister-pack will be non-narcotic medications that Dr. Cayen suggests you take as prescribed. The contents of the blister-pack depends on each patient’s medical history.
Taking the blister-pack of prescribed pain medications will help lower the amount of narcotics that you need after your surgery. Take the narcotic only as necessary, only if the blister-pack of pain medication is not adequate for your pain control. Narcotic pain medication can make you constipated, drowsy, nauseous and can be addictive. Many of our patients after hip and knee surgery don’t need any narcotics, if they take the blister-pack of pain medication as prescribed.
You will also receive a blood thinner medication to help prevent blood-clot for one month, if you are not already taking a blood thinner.
- Follow Up Appointments
You will see Dr. Cayen in follow up 1-2 weeks after your surgery in the Fracture Clinic. He will check your wound and make sure you are doing your home exercises.Your second follow up with Dr. Cayen will be at approximately the 6 week mark after your surgery in the Fracture Clinic. If you are feeling well at that point, no further follow up with Dr. Cayen is necessary unless concerns arise. If you have concerns regarding your hip replacement, please give Dr. Cayen’s Administrative Assistant a call.
- Wound Care
Before you leave the operating room, Dr. Cayen will place a water-proof bandage over your incision. You can shower with this bandage on. You will be instructed to take this bandage off 7 days after your surgery. More information about the dressing can be found here. You may replace the bandage with a strip dressing for showers, in order to keep the wound dry until the wound heals completely. Do not submerge the wound under water in a tub or swimming pool until the wound is completely closed (usually around 3 weeks after surgery).
- Driving
For right-leg surgery, you can drive once you are not using walking aids and are not using narcotics for pain control. For left-leg surgery, if you are driving an automatic transmission vehicle, you can drive once you are no longer taking narcotics for pain control. If you drive a standard transmission vehicle, the restrictions are similar to right-leg surgery.You need to feel confident that you can hit the break with good force and reaction time before you return to driving.
- Work and Activities
Return to work depends on the kind of job you have.
Sedentary/Desk job: It is reasonable to take 6 weeks off of a sedentary job after hip replacement. Many patients start working from home after a few days (as long as they are not taking narcotics for pain). Dr. Cayen suggests working not more than 2-3 hours per day during the first few weeks after surgery and to take frequent breaks. Sitting for long periods of time after joint replacement surgery can theoretically increase the risk of blood clots. Spend your first few weeks after surgery doing your physiotherapy and resting.
Walking Jobs: Typically patient can get back to an active job approximately 3 months after surgery. Many people have demonstrated return to work before that time. When you do return to work, Dr. Cayen suggests return to work gradually, with graduated hours and graduated duties over a number of weeks.
Manual labour: Historically, joint replacement surgery was reserved for the elderly and certainly those people who were not doing manual labour jobs. We do not have long term data on the effects of manual labour on joint replacement surgery however heavy lifting does place large forces through the joint. This could possibly lead to early loosening. Dr. Cayen does not recommend returning to a job requiring heaving lifting after joint replacement. If your are currently able to perform your duties in a job requiring heavy lifting, perhaps a joint replacement is not right for you at this time. You might want to hold off on joint replacement until after you are no longer able to perform heavy lifting, or discuss with your orthopaedic surgeon.
Most patients experience an improvement in their daily activities after they recover from hip replacement surgery. You are encouraged to resume non-impact activities after hip replacement. This can include, walking, cycling, elliptical training and golf. Many patients have returned to light tennis, skiing and even non-contact ice hockey/skating after their rehab is complete. As a general guide, if you can perform these activities without the risk of falling or loosing control (ie an expert hockey player or skier who takes it easy), then you may train and eventually return to that activity. Before you return to sport, it is imperative that your physiotherapist or athletic therapist guides your return to activity with a sport-specific exercise regimen, lest you risk injury.
It is not recommended that you return to high impact activities like jogging, running or jumping sports after joint replacement. Such activities cause high forces through the joint and can theoretically lead to early loosening of the components. Certain positions in Yoga and the use of an inversion table are not recommended after hip replacement surgery and these activities may increase the risk of hip dislocation.
- Dentist
For dental procedures, you do not need extra antibiotics above what is normally prescribed by your dentist. You should be in optimal dental health prior to your hip surgery. Infected teeth should be treated fully prior to your hip surgery. If you are approaching your scheduled regular dental cleaning, have that done prior to your hip surgery. Continue on your regular dental cleaning schedule after your hip surgery.
The Canadian Arthroplasty Society consensus statement for patient with total joint replacements having dental procedures can be found here. You may show this to your dentist.
- Travel and the Airport
Vacation travel after hip replacement can be done as soon as 6 weeks post operatively. Although it is possible to travel before then, it is recommended that they be short flights and that you get up out of your seat hourly to move.
For those who must travel prior to 6 weeks after surgery, blood thinner medication is recommended and can be discussed with Dr. Cayen or your family doctor.
Metal Detectors at the Airport:
You will likely set off metal detectors at the airport. You do not need a note from Dr. Cayen or your family doctor regarding your joint replacement. Just let the security personnel near the metal detector know. They may ask you to go through the body scanner instead. Given how common joint replacements are, security personnel are accustomed to this issue.
A video on metal detectors with joint replacements from the American Association of Hip and Knee Surgeons can be found here.
DISCLAIMER: The information on this website is intended to help current and prospective patients of Dr. Cayen understand joint disease as well as treatment options available. It is also meant to provide background information to prospective patients such that their visit with their doctor is most helpful. This website is not meant to provide specific medical advice, treat or diagnose any medical condition. It is not meant to take the place of a visit with your doctor or Dr. Cayen.
About Dr. Cayen
Dr. Barry Cayen is an orthopedic surgeon at Humber River Hospital, specializing in adult hip and knee replacements, sports surgery of the knee, and trauma. He performs Total Hip Replacement Surgery using the Direct Anterior approach with a Hana table.